Disability: Models, Cultures, Perceptions and the Path to Inclusivity.
Understand more about the models, cultures, stereotypes, and language surrounding disability, and how we can move towards a more accessible and inclusive society for all.
Disability is a famously loaded term. It lies awkwardly at the intersection of biology, identity, and society. It’s hard to talk about in a general way because it means many different things to many different people. Around 20% of people are in some way disabled — that’s 1.5 billion across the globe, so it makes sense that any given statement about disability will attract disagreement. In this article, I’m going to attempt to uncover what we mean when we say ‘disabled’, the challenges endured by disabled people, how the cultures and stereotypes of disability present in modern times, and finally how we can move towards a more inclusively designed society that takes into account everyone's needs.
Why am I writing this? In 2019, at the age of 29, I suffered a stroke that left me partially paralyzed and disabled. I’m writing this article, in part, to understand my own disability, and also to communicate the things I’ve witnessed as being rarely understood by the mainstream about disability. I’m also writing it with the hope to forward the cause of inclusivity and equality for disabled individuals.
The very first thing to know is that there are traditionally two competing models in how we define disability: the older medical model and the newer and more accepted social model. Let’s explore these.
The Medical Model
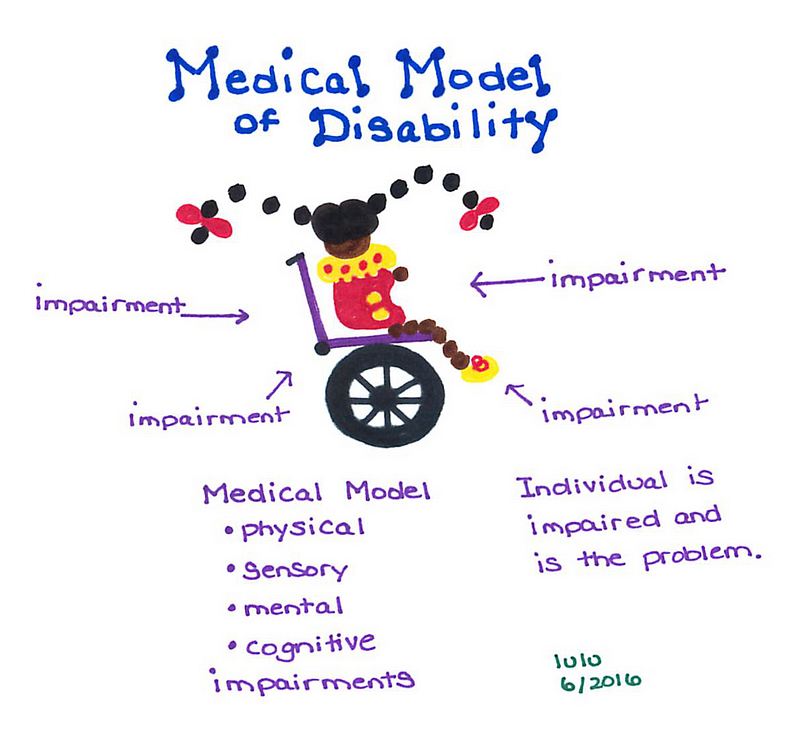
The Medical Model of Disability (Image by SeekFreaks)
The medical model says we are disabled by pathology: i.e. disease processes and disorders of the body. This model tends to focus on individual accommodations instead of societally-endemic issues, and can result in increased stigmatization due to its “us and them” paradigm. It also is seen as giving power to authority as it lets medical institutions paternalistically define disability as a “problem” to be solved.
(From Wikipedia) The medical model of disability, or medical model, arose from the biomedical perception of disability. This model links a disability diagnosis to an individual’s physical body. The model supposes that this disability may reduce the individual’s quality of life and the aim is, with medical intervention, this disability will be diminished or corrected. The medical model focuses on curing or managing illness or disability. By extension, the medical model supposes a “compassionate” or just society invests resources in health care and related services in an attempt to cure or manage disabilities medically. This is in an aim to expand functionality and/or improve functioning, and to allow disabled persons a more “normal” life. The medical profession’s responsibility and potential in this area is seen as central.
There has, at times, been contentious debate and even animosity towards the medical community due to how “problems” or “deviations” are identified. Who gets to say that something is a “disorder” vs. an ordered & evolved difference? Like all of disability, it is a muddy and complex space where identity, medicine, and culture are all in the mix.
Book Tip: Read Far From the Tree by Andrew Solomon to get a grasp of how supposed disabilities and disorders, such as deafness and dwarfism, relate to identity, and how some of these individuals reject the medical model of their difference.
The medical model of disability is criticized for not taking into account the environmental and social factors that heavily influence the degree of a disability. Because of this, it has been blamed for giving our governments, employers, and wider society a license to ignore disability and let it be “handled” by medical professionals, stealing opportunities of social and economic participation from disabled individuals by keeping them “contained” and “accommodated” in specifically designed spaces.
The Social Model
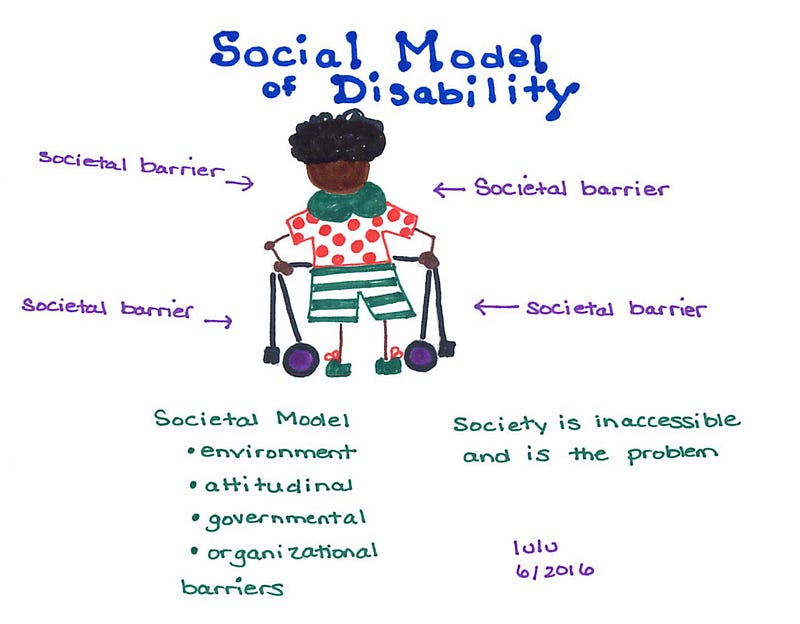
The Social Model of Disability (Image by SeekFreaks)
The social model says that we are disabled by the world and its lacking understandings, practices, and infrastructure. It is a model more supported by disabled individuals and organizations. It focuses not on deficits in individuals, but on deficits in society.
(From Wikipedia) The social model of disability identifies systemic barriers, derogatory attitudes, and social exclusion (intentional or inadvertent), which make it difficult or impossible for individuals with impairments to attain their valued functionings. The social model of disability diverges from the dominant medical model of disability, which is a functional analysis of the body as a machine to be fixed in order to conform with normative values. While physical, sensory, intellectual, or psychological variations may cause individual functional limitation or impairments, these do not necessarily have to lead to disability unless society fails to take account of and include people regardless of their individual differences.
The social model enables us to see and fix the underlying problems in society that are disabling people. This is everything from our transport infrastructure to our expectations around social participation. The social and economic fabric of society is currently built in a way that expects a narrow and specific body type and mind, and limits the participation of not only physically disabled individuals but also those with cognitive differences, mental illnesses, and learning difficulties.
The social model sees the failure in society — not in the human. And it tasks us — all of us — to re-think and re-design the spaces and processes that we have influence over.
Bridging the medical and the social
The social model and the medical model have often competed, and over time the medical model has been invalidated as the primary lens through which we view disability. However, the social model is not without its own limitations. For example, it does not fully account for the types of daily challenges and impossibilities faced by those with very severe illnesses or impairments, such as those that completely limit ones’ ability to feed oneself, clean oneself or communicate in any way. Fundamentally, the social model fails to see illness as at all related to the concept of disability.
At the very least, we can all agree that disability alludes to a deficit of some type, but whose deficit is it? Is ‘disabled’ something we are or something that society does to us? Is it a medical condition or an oppressive force? A permanent attribute or a passing fluctuation?
The “International Classification of Functioning, Disability, and Health” (ICFa.k.a. ICIDH-2), published by the World Health Organisation (WHO), broadly sets out a model of disability based on:
Things within or of the body: the differences in structure or function of the body when compared to either what is “normal” or what is medically “healthy”.
Things outside the body: the environment, society, economic circumstances, cultures, attitudes, services, and policies that we are exposed to in our everyday lives.
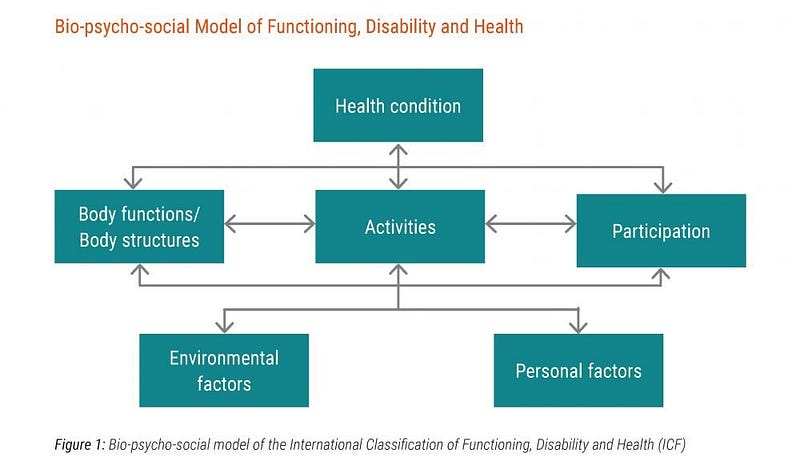
Within the ICF, WHO adopts the Bio-psycho-social model of disability. This model proposes that neither the medical nor social models are sufficient, as disability is a function of many biological, psychological and social factors.
The Bio-psycho-social Model
A diagram showing the “Bio-Psycho-Social model” of disability as defined by WHO.
Within the ICF, the bio-psycho-social model is broken down into six elements that, together, dictate how able a given person is to carry out an action. This may seem very granular but we need to appreciate all of these elements if we’re to fully understand disability.
Inside (or of) the body, we have:
Health Conditions: anymedicaldiagnoses, disorders or diseases.
Body Functions & Structures: organs, limbs and components and the functions they provide.
Outside the body, we have:
Environmental Factors: the physical and social space we inhabit, including people, attitudes, cultures, laws, geography, and more.
Personal Factors: things like gender, coping styles, social background, education, profession, experiences, character etc.
And finally, there’s “Participation” which, in WHO-language, is basically… everything that you may want to do in the universe,… including regular habits like hoovering cat hair, chatting to your neighbor, getting a job, or visiting the ISS.
All of these elements come together, at any given moment, to give us the last element, what WHO calls an “Activity”. This is the actual granular doing of the thing. It sits at the center of all of these pieces and is the true test of how abled or disabled we are in any given moment or context.
An example…
Let’s try stringing all these pieces together into an example. I’ll use myself since I know what my disability means for me.
I have left-side-weakness, neuro-fatigue and epilepsy due to a brain injury; I’m 30 years old, asthmatic, hypertensive, male, live in London and work as a software engineer; I want to go shopping for groceries today.
This brief description speaks to all elements.
Participation: in the act of shopping.
Health Condition(s): brain injury, epilepsy, asthma, high blood pressure. Otherwise good health.
Body Structure & Function: normal except for neurological bruising, left-side-weakness (slow walker!), and neuro-fatigue.
Environmental Factors: where my home is, where the shop is, the weather, the topography, noises, sights, other people, the social schema of being in public, the structure and layout of streets and shops, regulations and expectations around how to act in a shopping environment. Etc.
Personal Factors: do I know where the shop is, can I afford it, and do any of my other characteristics (my job, my appearance, my ethnicity, my privileges, my gender, etc.) factor into the difficulty of navigating there by myself and participating in the act of shopping? Etc.
Activities: waking up, getting dressed, putting shoes on, grabbing my stick, walking to the shop, navigating the pavement, putting on a mask, holding a basket, finding and picking up items, queueing, operating a checkout machine, etc.
Combining all these elements, the ICF gives us three ways of defining moment-to-moment disability:
Impairment: a problem in body function or structure such as a significant deviation or loss. E.g. weak left-side.
Activity Limitation is a difficulty an individual may have in executing an activity. E.g. Slow to reach items on lower shelves.
Participation Restriction is a problem an individual may experience in involvement in life situations. E.g. food items on lower shelves are less accessible due to the *design of the shop*.
This triad allows us to see how disability presents in non-obvious ways. For example, a pregnant person, while typically not considered disabled, may still be unable to do certain things. While some of these will be due to activity limitations (e.g. putting on trousers with ease), others may solely be due to participation restrictions (e.g. disallowed from a theme-park ride). Usually, however, disabilities involve every aspect of the triad.
So, that’s a summary of the bio-psycho-social model. As dull as it may seem, it’s a very useful template that we can use to identify how disabilities manifest, and even how they may present in people who do not consider themselves “disabled”. In my opinion, it nicely bridges the advantages of both the social and medical models of disability.
Disability: perception vs. reality
For many, disability is seen as synonymous with mobility challenges. Perhaps this is why the popular symbol of disability is a person using a wheelchair. But only half of disabilities actually involve such challenges, and even fewer involve the need for a wheelchair (only ~11% of all disabilities).
Only 11% of disabilities involve the use of a wheelchair. Photo by Julius Carmine on Unsplash.
The bulk of disabilities are invisible. In addition, many disabilities aren’t always present to the same degree. A person may struggle or require an aid when experiencing flare-ups, fatigue, and other fluctuations, but may be perfectly fine without any adjustments or aids at other times. And what we see of disability — in the public sphere — is usually the more functional side, and not fully representative of the struggles:
“When you see someone with ME [myalgic encephalomyelitis], you see them when they are on a good day or at a good point. You don’t see the fact that they have been lying down and resting for two days before and then they will have to do the same to recover afterwards. People just don’t get it.” (Female with a long-term illness, London)
— EHRC: “Opening up work: The views of disabled people and people with long-term health conditions” [pdf]
Disability is not static; within individuals, it changes from hour to hour, day to day, year to year. The mainstream may expect, for example, all wheelchair users to always require their wheelchair. But a significant chunk of wheelchair users can walk, but at great expense, and so they carefully choose what aids they need in order to navigate each part of their day with less exhaustion, pain, or other symptoms.
Many suggested I was faking and would express their disgust. This had a detrimental effect on my self esteem and I stopped going out because I feared being judged. I want people to know that using a wheelchair allows me to get around easily without excessive pain. Please when you see a wheelchair user walking please don’t immediately assume they are faking. There are many disabilities that are invisible or present with intermittent weakness — Emerald, 29, Mitochondrial Myopathy
Not every disability is obvious or visible
The visible markers of disability on a given person are rarely a comprehensive indicator of their challenges. A wheelchair user’s mobility challenges may in-fact be the least of their concern.
These many incorrect perceptions can only be solved by advocacy and education.
There is a lot to be said for the language we use, as well. Language drives meaning & understanding, so let’s explore how language intertwines with disability.
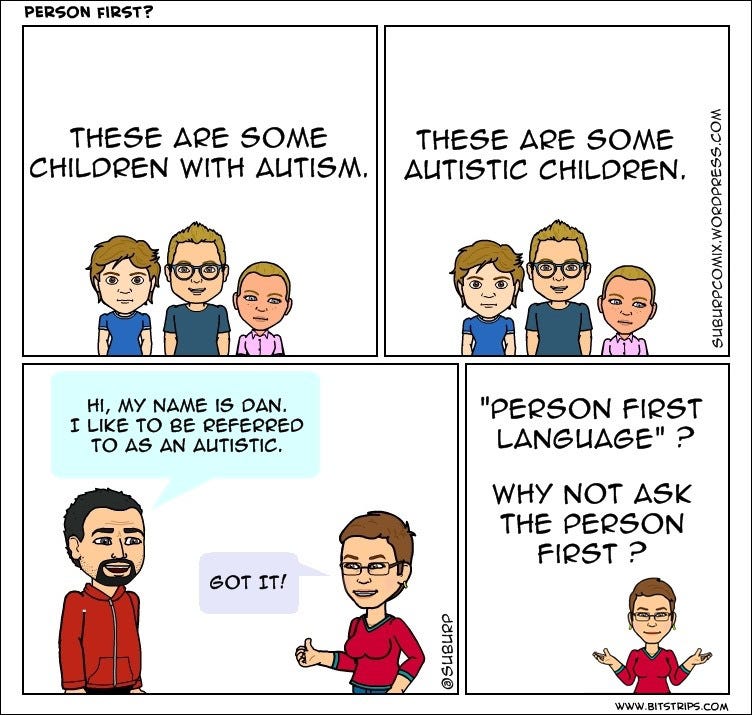
Language & Terminology
There is always debate around what kind of language we should use to describe disabled individuals. The person-first approach says we are each a “person with disability” (PWDs), as opposed to a “disabled person”.
However saying “person with X disability” is criticized as it can cast the disability as an undesired or inconsequential trait, much like a passing sickness. “Disabled person”, in contrast, communicates that disability is not a secondary or negative trait but a vital part of identity that can affect every part of ones’ life, not unlike sexuality or ethnicity.
Identity-oriented language like “disabled person” can also let us see disability as not a negative deficit in the person but a shame-free trait that is borne of environmental factors and systemic ableism: i.e. the social model: we are not people with disability; it is society that disables us. Compare seeing disability as something “within them”, as opposed to seeing it as a thing “cast upon them” by society.
The language we use becomes more complex when referring to pathologies that have manifested as disabilities at some point in one’s life (e.g. cancer or a broken leg). In many cases, people prefer to hold these as traits, not identities. This is especially true of illnesses where there is an expectation or culture of recovery. E.g., it is usually preferred to say “person with a mental illness” rather than a “mentally-ill person”. The latter seems to encapsulate the whole of the person under a trait as if it permanently defines them instead of just being something incidental to their identity and character. However, it also arguably disregards the impact that mental illness can have on a person. At times such illness may be all-encompassing to an extent that “person with X mental illness” seems invalidating or minimizing.
There are some cases, as well, where people may be reluctant to communicate their disability or illness, either as a core part of their identity or as a trait because of stigmatization around it. Many sexually-transmitted diseases and mental illnesses are affected by such stigma.
There are additionally people with conditions or differences that may prefer to avoid medical definitions altogether and use more positive and identity-oriented language, especially in cases where there is a strong in-group culture. An example of this is the term “aspie” which is used by some people with Asperger’s syndrome. There are also developing terminologies around neurodiversity (“NDs”) and neurotypicality (“NTs”) amongst people with autism and other neurological differences. Communities tend to coalesce around language that enables them to communicate in a shame-free way, and this often means rejecting the person-first approach. This is ironic because the person-first approach is often assumed by the mainstream to be more dignified and sensitive, but it often ends up being the opposite.
In the autism community, many self-advocates and their allies prefer terminology such as “Autistic,” “Autistic person,” or “Autistic individual” because we understand autism as an inherent part of an individual’s identity…It is impossible to affirm the value and worth of an Autistic person without recognizing his or her identity as an Autistic person. Referring to me as “a person with autism,” or “an individual with ASD” demeans who I am because it denies who I am…When we say “person with autism,” we say that it is unfortunate and an accident that a person is Autistic. — Lydia Brown
In-group language may also refer to people outside the group. For example, the term “allistic” is sometimes used by those with autism to describe those without autism — sometimes in a tongue-in-cheek manner.
There are also in-group labels used in survivor communities, such as “strokey” (a stroke survivor). Such a term is used as a means of community and affection, however, it may be seen as derogatory if used by non-stroke-survivors.
The simplest and best way to form language around disability is to simply ask the person or community you’re referring to. It’s vital to understand that identifying language may be sensitive to who is saying it and the context in which it is said. There are strong cultures and communities that may use language internally (reclaiming ownership of language) that may be seen as derogatory when used by others. The best policy, as ever, is to ask. And, of course, never assume you know a person, their condition, their disability, or their identity better than they do.
Non-disabled people shouldn’t lecture disabled people on correct terminology. Almost no term is as insulting as a non-disabled person patiently or aggressively explaining to a disabled person why their own way of talking about themselves is wrong. The rules and implications of disability language are always evolving. They don’t shift and change just to mess up nervous non-disabled people. They change as disabled people’s understanding of ourselves and our place in society changes, and as our aspirations change as well. — Andrew Pulrang
More reading on the matter of disability language:
The legacy of disability perception and the stories often told are littered with inhumanity, indignity, and ignorance. The mainstream has often been criticized for reducing disability into so-called inspiration or tragedy “porn”. Disabled people are celebrated or held up as a vessel of awe, sympathy, and sorrow, satisfying the need of some to project an affectation of humility and gratitude when reflecting upon their own “blessed lives” or “ableness”:
[Disability tragedy porn] is a particular type of narrative about disability that can appear in fiction and nonfiction, in a wide variety of media. It conceptualises disability in a very specific way, tragedising the lived experience of disabled people and underscoring the idea that disability is the worst thing ever, the most awful imaginable thing that could happen to someone. It collapses all disabled experiences into one umbrella of misery. — Disability Tragedy Porn, Defined (s.e. smith)
“It’s a portrayal of people with disabilities as one-dimensional saints who only exist to warm the hearts and open the minds of able-bodied people” — Speechless
Disabled lives are lived against a backdrop of systemic ableism, meaning that a disabled individual often has to work harder than a non-disabled individual to reach the same milestones in a society that is not made for them.
But this does not mean that we should assume a certain level of hardship or blindly hold up disabled people as examples of resilience or perseverance. Every person is unique, with their own challenges and circumstances. And so every person deserves to have their story understood and told in a way that respects their truth: the positive, the mundane, and the negative. Disabled individuals are as imperfect as anyone else. Placing them on a pedestal is disingenuous and reduces real humans to fake but satisfying virtues.
When a space or part of life is unaccommodating, disabled individuals are less able to be there, thus not seen to be there, and therefore not thought about or catered to in the design of those spaces and processes. It’s a neverending cycle of disempowerment and invisibility unless crucial interventions are made.
Over time the disability rights movement has had to fight hard to bring changes in accommodations, from disabled toilets to wheelchair-ramps. Legislation has, in many places, now been implemented. It often sets out what adjustments public and private organizations must provide.
With these advancements in mainstream understanding and accommodation, disabled individuals across the spectrum have been able to navigate more easily and partake more in public and economic life. However, there is still vast inequality across the globe.
Disability Rights are Lagging Behind
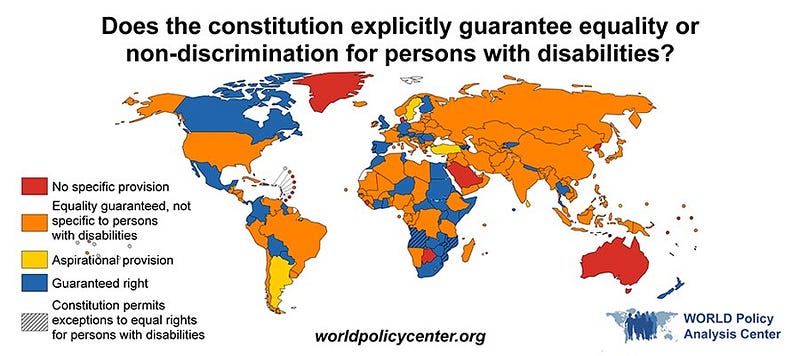
Since its first adoption in 2006, 182 countries have become signatories to the UN’s Convention on the Rights of Persons with Disabilities (CRPD). This treaty requires signatories to promote, protect, and ensure the full enjoyment of human rights by persons with disabilities and ensure that persons with disabilities enjoy full equality under the law.
Many of the signatory countries, however, have still not taken sufficient steps. In 2019, the World Policy Center prepared a report that showed how, among countries that have ratified the CRPD, only 27% of their constitutions explicitly guaranteed equality or nondiscrimination on the basis of disability.
It is not sufficient to be a signatory to such a treaty; in a way it means nothing. Such treaties need to be manifested in each country’s legislation otherwise it has little effect.
Constitutional rights can be powerful tools to reverse discriminatory laws and policies, shift social norms toward inclusion and more.Yet, guarantees to persons with disabilities still lag behind those extended to other groups, even among more recently adopted constitutions. Between 2010 and 2017, 100% of new constitutions explicitly guaranteed equality on the basis of gender, as did 92% on the basis of religion and 79% on the basis of race/ethnicity — compared to 71% on the basis of disability.
The history of disability equality across the globe is a sad one, but treaties like the CRPD, although facing slow adoption, are powerful forces that will hopefully continue to push nations to constitutionally protect all disabled citizens.
However, this is still an ongoing fight in many countries. For example, the US Senate has still failed to ratify the CRPD, apparently, in part, because it would cast into shocking light the lacking provisions of the ‘Americans with Disabilities Act (ADA) of 1990'.
A story that reveals itself the world over is the empowerment that comes from the ability to economically participate. Many take it for granted, but where economic participation has historically been inaccessible (whether due to gender, ethnicity, migrant status, etc.) any newfound economic access, for example via employment, yields a tonne of social mobility and improved economies.
Economic Participation & Employment
Both the disability unemployment rate and the pay gap are staggering and in some places, like the UK, are increasing. The isolation due to this lack of participation creates observable negative effects on physical and mental health. Disabled people more often end up in food poverty, have less access to education, are more likely to experience hate crime or harassment, and have more issues with housing and transport.
It’s not just an adequately budgeted healthcare and welfare system that we need, but a focus on economic participation. Empowering disabled people with the same economic choices and freedoms as non-disabled individuals is a hugely impactful way to reduce inequality.
“Work confers important benefits. It provides opportunity for purposeful activity, for financial independence, for social inclusion and social status.” — Dr Lisa Cameron MP (The All Party Parliamentary Group on Disability)
Participation, however, is not enough. It must be equal, dignified, and non-exploitative. But that is rarely the case. The history of disabled exploitation still bleeds into the present day. In the US, firms are still legally allowed to pay sub-minimum wages based on ability and productivity.
Out of the small population of people with disabilities who are hired, many receive sub-minimum wages. In recent years, there have been reports of an estimated 420,000 individuals with disabilities who have been paid an average of just $2.15 per hour. — Forbes
If we are to get higher numbers of disabled people into jobs and participating equally in public life, the oft-cited “low friction” adjustments, like a new desk chair or longer work breaks, won’t be enough. It is true, such adjustments were hard-won in decades past and there are now many legislated duties across the globe for employers to “make such reasonable adjustments” (UK Equality Act 2010). But how far do these duties extend? And what even are “reasonable adjustments” and, crucially, do they occur?
Employers have duties to make adjustments for their disabled employees, but is this enough? Do employees actually end up getting the adjustments they require? (Image by Nadia Bormotova Source)
There’s evidence that, often, adjustments are not even asked for:
Individuals felt that the personal risk involved in requesting any form of adjustment to their work arrangements was not worth taking. They feared that articulating a need outside the mainstream would lead to them being viewed as ‘causing problems’ or being ‘unable to cope’ in management eyes and also open them up to accusations of ‘special treatment’ from colleagues. The fact that any form of disclosure of need could never be ‘taken back’ once made led most participants in the research to conclude that it was better to ‘struggle on’ and develop coping mechanisms even if this meant they were ultimately less productive at work than they could be.
— EHRC: “Opening up work: The views of disabled people and people with long-term health conditions” [pdf]
Not only are there barriers to disclosing a need for adjustments, but the process itself can be a long-winded and stressful exercise in self-advocacy:
Negotiations for accommodations can be arduous, even when they are conducted in good faith. When Charis Hill asked for a yoga ball chair to alleviate pain related to their ankylosing spondylitis, a type of arthritis that affects the spine, a simple request stretched into weeks of public self-advocacy. “I felt a little humiliated by the lack of confidentiality when the time came to complete the formal request,” they said. “The experience certainly made me have second thoughts about requesting any other assistance in order to do my job.”
Some have likened the experience of disclosing one’s hidden disability to that of “coming out”. There’s an additional stigma to disclosing specific illnesses, as well, such as mental illness or any disabilities with emotional or atypical behavioral symptoms (source). This disclosing process places a great burden on the disabled individual, asking them to vulnerably reveal their differences and challenges to a depended-upon and powerful authority, as if seeking charity or judgment.
The whole idea of disclosure and adjustment reflects and adds legitimacy to the model of society that we are adjusting to, i.e. the same society that is disabling us. This is how structural ableism subtly presents itself. It says to us that “you need slight adjustments in order to fulfill the unchanged demands of employment” but it does not seek to change or adapt those demands of employment. This is the crux of the problem with any adjustment: its intent is only to gently alter but never change any fundamental aspect of the job itself.
There’s rarely a shallow-end for integration. It’s all-in or all-out. So if you can’t fulfill expectations you’re often not wanted and not seen. Invisibly invisible, and back to a never-ending “convalescence”.
Broken Stereotypes & Incentives
We place a considerable duty on employers to help close the gap and deliver more equality to disabled people. But employers are simply not willing or able to solve this on their own. Outside of direct (non-structural) discrimination, there are specific factors of reluctance that tell us why a given employer may not choose to hire or accommodate disabled individuals:
Incorrect Beliefs regarding competence, temperament, and attitudes. These beliefs are rarely substantiated by the evidence and often due to a lack of exposure to actual disabled individuals.
Lacking Incentives (and dis-incentives) to hire minorities such as subsidies, levies, tax breaks, loans, employer assistance (etc.) are all sorely lacking in many countries.
Lacking Opportunity: due to the current inequality and ableism in society, disabled individuals are statistically less likely to have been afforded the same level of education as non-disabled people, thus they are left less able to meritocratically (by the asset of their talents, skills, and accrued knowledge) find employment.
Fear of the Unknown: as well as being simply ignorant of the nature and diversity of disability, employers may also be worried about handling things incorrectly, lawsuits, or internal disputes around special treatment.
A vital part of closing the employment gap is bringing any incorrect perceptions of disability more inline with the reality of disability. Carrying broken stereotypes is damaging and manifests in many different ways. Here’s just one, referencing a common misconception of those who are hearing-impaired:
Observers may classify a hearing-impaired (i.e., deaf) person as incapable of performing the job of a supervisor because the job requires face-to-face communication and the ability to communicate with others on a telephone. The reason for this is that the prototypical hearing-impaired person cannot understand or orally communicate with others. This inference, however, may be incorrect about a particular hearing-impaired person who has the ability to read lips and communicate orally with others. (Stone and Colella, 1996) (ref)
Currently, disabled people who have been able to find work are generally experiencing less job satisfaction, less well-being, and less fairness from managers (source). This drastically diminishes their ongoing faith in the job market, as well.
In search of more diverse workforces, better recruitment practices are often cited. And it is, indeed, important to improve the funneling and recruitment process for disabled individuals (see how here), but that is not enough. We have to create new roles and hybridize existing roles such that the workplace becomes accommodating to the full gamut of human disabilities and differences.
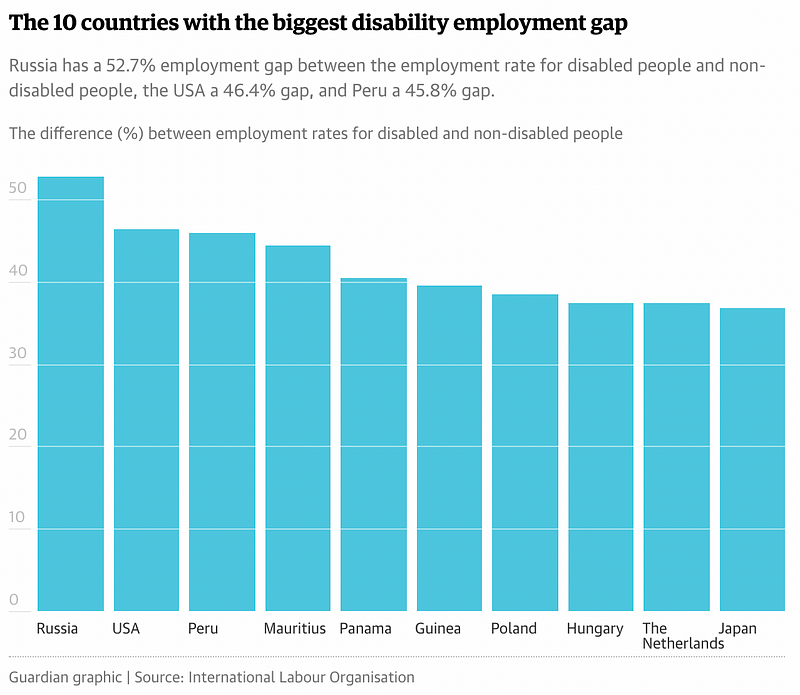
Do employment quotas work?
The evidence shows us that one of the most effective ways of bridging the employment gap — and creating more accommodating working practices — is via legislated quota systems. Countries without such quota systems tend to have the most extreme employment gaps (source):
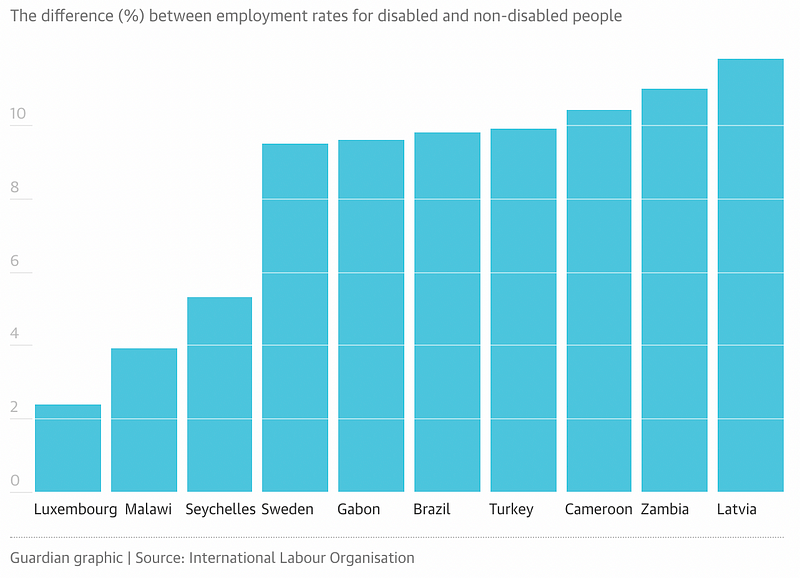
Whereas countries like Luxembourg have long-standing quota systems. And we can plainly see the results:
The quota approach has proved itself in other countries including Austria, France, Italy, and Spain. But it is clear that the mere presence of quotas is not enough. It needs to be combined with:
Strong incentives (e.g. subsidies) to drive hiring.
Strong disincentives (e.g. levies) to dissuade apathy.
Strong legislation around anti-discrimination, specific duties of employers, and employees alike (e.g. whistleblowing)
A recognition that the level of accessibility and opportunity is different across the spectrum of disability, so any legislation or inclusion efforts need to ensure that every level of acuity and diversity is represented.
A strong culture of inclusivity in every organization, driven by HR, recruitment, and internal panels of diversity and inclusion (D&I)
It is clear that an approach based purely on anti-discrimination laws, workplace accommodations, and voluntary employer-led programs is insufficient. A quota-based approach is needed. If more countries chose to introduce such quotas they’d likely experience a positive virtuous cycle:
The hiring of disabled individuals increases due to legislated quotas.
Thus disabled people have more disposable income, economic freedoms, and representation in the public and work sphere.
Thus difficulties and lacking adjustments are plainly observed and identified by both the non-disabled and disabled.
Thus improved accommodations, better systemic design, and further legislative change is driven.
Thus disabled workers can increasingly and more meritocratically partake in the economy of jobs & other parts of life.
Rinse, Repeat (until equality…)
Building Inclusivity into Society
The lacking economic participation amongst disabled people is not due to the severity of their deficits. It is due to the unaccommodating structures and processes of participation that exist. The ways that people lead economically & socially fulfilling lives are simply not as available to disabled people.
For some, the way society works allows them to glide through it like water, whereas for others, most often those who are minorities or disenfranchised due to the bend of history, it can be much more like swimming through treacle or jam. This treacle can be likened to the “environmental factors” within the bio-psycho-social model.
Unnaccommodating situations are the treacle that disabled people must swim through every day. In order to change that treacle to water, we have to undertake a huge process of re-thinking and re-designing. We need to think about:
How we design events, pick locations, and structure agendas.
The facilities we choose to build (from disabled toilets to sensory rooms).
Common expectations about workload, tasks, deadlines, scheduling, speed, and the quantities and types of people needed for any given task.
Design of government and private application processes: e.g. filling out complex forms or providing proof of disability.
Design of transport infrastructure: access, cognitive complexity, etc.
Design of home appliances and electronic goods: size, intuitiveness, clarity, readability, interface design (visual, sound, touch, braille). Etc.
Dimensions and materials of doorways, corridors, aisles, seating, …
Designing for sensory needs, navigation needs, cognition needs, …
Inclusive and accessible technology, including websites, apps, and newer tech like Virtual and Augmented reality.
Etc.
In the long term, it is far more equitable, dignified, and efficient for businesses and beneficiaries alike, to re-think and adapt the design of inaccessible things rather than creating often undignified parallel systems just for disabled people.
The best examples of inclusive design don’t shout ‘inclusive’; they just happen to embrace a really wide range of users. — Mat, Design Council
By instilling a new standard of design across the board, we can bring about more participation in economic and public life not only amongst disabled individuals, but amongst the neurodivergent, parents, carers, the elderly, the young, the highly-sensitive, and so many more people who are shoved to the sidelines of society.
Building true accessibility into the fabric of society is no easy task. It requires fresh-canvas thinking and an approach that centers on the uniqueness and dignity of each person. Accessibility is not a singular trait; it encompasses many different affordances and use-cases from across the spectrum of disability.
To give you an idea, here are some specific examples of how we might bring broader accessibility to our processes and structures:
Designing all spaces used by the general populous to be fully accessible. This would include waiting areas, ALL toilets, and thoroughfares. I.e. no haphazardly implemented half-measures or “your place is over here” approach to disabilities.
Eliminating all narrow areas, stairs, severe inclines in the design of building entrances & exits (this includes fire exits!)
Having every doorway, aisle, and corridor wide enough for a mobility device to navigate (moving forward, backward, turning) without demanding dextrous control of interfaces or objects (e.g. doorknobs or complex entry systems).
Making all user-interfaces fully accessible (a11y) & sensitive to sensory challenges, different types of blindness, hearing impairments, etc.
Implementing seating, rest areas, and coves along all pavements, trails, corridors, and in large or overwhelming gathering spaces.
Architecting spaces and urban environments so that navigation difficulty, cognitive complexity, and sensory overwhelm are minimized.
Making education and working hours flex to the needs of all, whether those be needs of disability, parenting, illness, caring, appointments, or even grocery shopping. I.e. fitting work around life.
Making all educational curriculums accommodate the full diversity of interests, passions, learning styles, needs, and competencies that exist. For example, doing away with long lecture-sessions that end up disproportionately punishing those with disabilities.
Providing multiple ways of absorbing every piece of information: spoken, written, visual, conveyed via sign language, braille, closed-captioning, other languages, and simplified language catering to cognitive/intellectual divergences and disabilities.
Enabling people to partake in both online and offline events after they have occurred. Many disabilities involve fluctuations in pain and fatigue that cannot be foreseen.
Putting dignity at the core of any adjustments that require specific attention or assistance. I.e. designs of structures or processes should not create an uncomfortable spectacle of an individual.
(plus so so so many others) …
It may seem a utopian dream that we can design the world around us such that it accommodates the full diversity of humankind, but it truly is the baseline of what we should expect. If 20% of us are disabled, then we should bias to seek 20% representation and presence in every area of life. And with a focus on inclusive design and a fuller understanding of disability, we can achieve this.
Thank you for reading!
I hope you’ve come away with new insights about the fuzzy, chaotic, and ever-changing models and issues surrounding disability. I would have loved to cover so much more, but instead, I’ll leave you with some useful resources, articles, and books: